
About CAIRHE
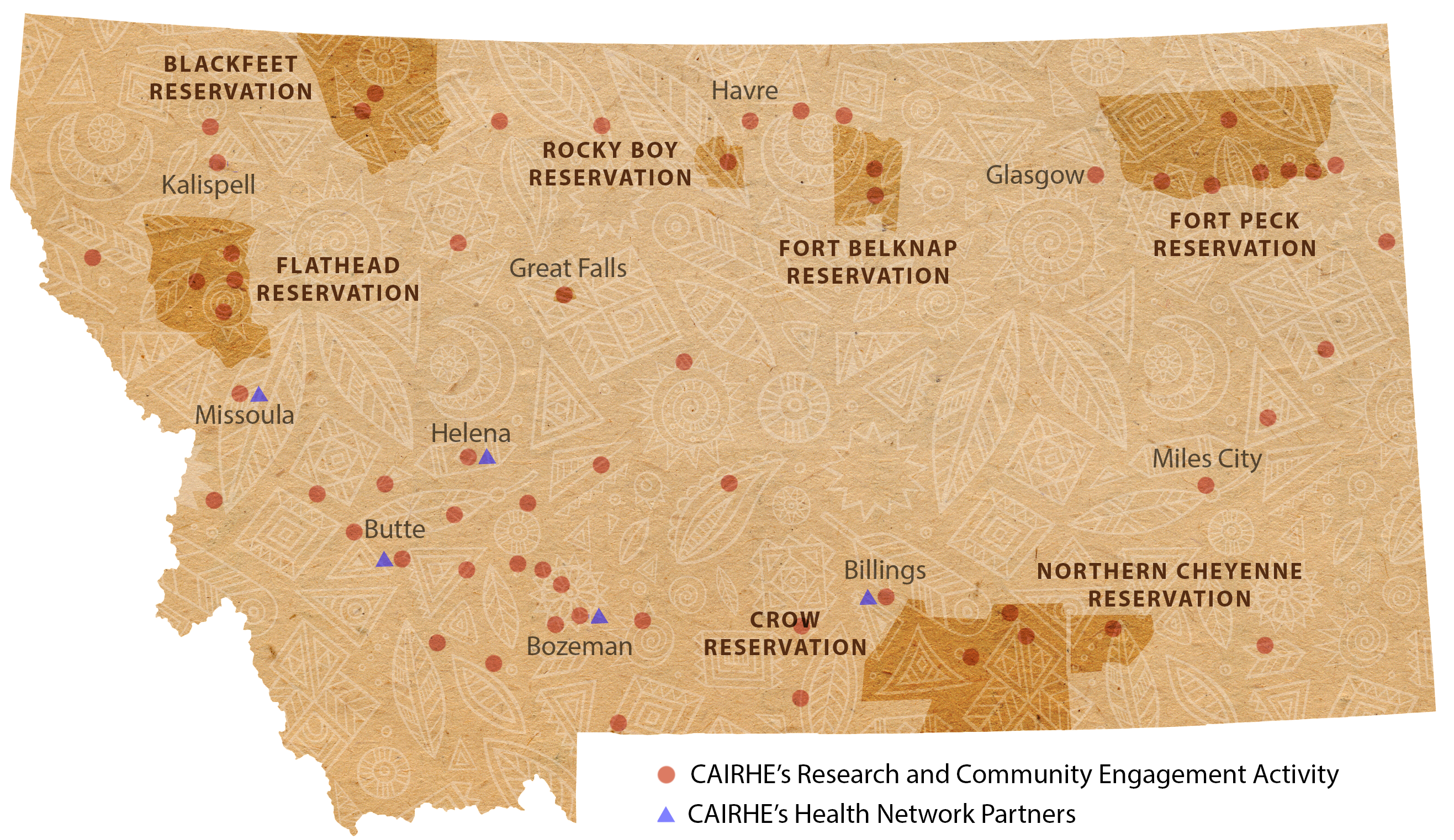 The locations of CAIRHE's research and engagement efforts continue to expand across
Montana. (Map by Kristen Drumheller)
The locations of CAIRHE's research and engagement efforts continue to expand across
Montana. (Map by Kristen Drumheller)
Based at Montana State University, CAIRHE (“Care”) is an official state of Montana research center designated by the Montana University System Board of Regents.
CAIRHE's mission is to reduce significant health differences in rural communities through community-based participatory research (CBPR). CAIRHE serves the people of Montana as a robust, interdisciplinary research center with strong engagement in communities across the state (see map above). Using proven CBPR methods, the Center and its investigators conduct groundbreaking health research and interventions that make a profound, sustainable difference in the lives of Montanans. CAIRHE also maintains a growing statewide and national network of research partners, including clinical organizations, public health agencies, foundations, and other centers, as a way to expand collaboration and dissemination of positive research outcomes.
Montana is a profoundly rural state in the most sparsely populated region of the United States. More than 34 percent of Montana’s residents live in rural areas, the highest percentage of any state, and Montana and its neighboring states (Idaho, Wyoming, South Dakota, and North Dakota) have 5 of the 7 lowest population densities in the United States. Rural risk factors for health in Montana include geographic isolation, fewer health care providers, higher rates of health risk behaviors (such as binge drinking, driving under the influence, and unhealthy diets), lower socioeconomic status, and limited employment opportunities. According to the Montana Department of Public Health & Human Services, residents of rural Montana counties have higher mortality rates for 6 of the 10 leading causes of death, including heart disease, diabetes, and chronic liver disease and cirrhosis, compared to residents of more urban counties.
CAIRHE is working hard to reverse these trends. Building on recent achievements, CAIRHE will continue to serve as the catalyst for original and innovative multidisciplinary research and community collaborations that will have significant impact on health in our underserved region.
About CAIRHE Director and Principal Investigator Alexandra Adams, M.D., Ph.D.
 Alex Adams is Director and PI of CAIRHE, a position she has held since 2016. The foundation
for all of her leadership and research has been community-based participatory research
(CBPR), working in partnership with communities to understand and solve health challenges
using both scientific rigor and crucial community knowledge. She has directed multiple
clinical trials, including the Healthy Children Strong Families 2 trial in five tribal communities nationally, and has more than 60 peer-reviewed publications.
She has held K23, U01, U54, R01, P60, P20, and P30 funding from the NIH, as well as
more than $10 million in foundation funding. In October 2021, Dr. Adams was elected
to membership in the National Academy of Medicine.
Alex Adams is Director and PI of CAIRHE, a position she has held since 2016. The foundation
for all of her leadership and research has been community-based participatory research
(CBPR), working in partnership with communities to understand and solve health challenges
using both scientific rigor and crucial community knowledge. She has directed multiple
clinical trials, including the Healthy Children Strong Families 2 trial in five tribal communities nationally, and has more than 60 peer-reviewed publications.
She has held K23, U01, U54, R01, P60, P20, and P30 funding from the NIH, as well as
more than $10 million in foundation funding. In October 2021, Dr. Adams was elected
to membership in the National Academy of Medicine.
CAIRHE is supported by a Centers of Biomedical Research Excellence (COBRE) award from the National Institute of General Medical Sciences of the National Institutes of Health (P30GM154593), among other grants.
